
Stopping myopia progression through proactive myopia control strategy with Ortho-K and 0.05% atropine combination treatment and lifestyle adjustment.
A year and a half ago, I began sharing my personal insights about my son’s myopia control journey, offering a glimpse into what I've learned about stopping myopia progression and the challenges of finding a suitable local doctor in the US. Jump to the present, and I'm thrilled to provide an update on the remarkable progress we've made in managing my son's myopia. Whether you and your child are just starting or have already embarked on a myopia control journey, I invite you to read about our experience and learning.
A year and a half into our myopia journey
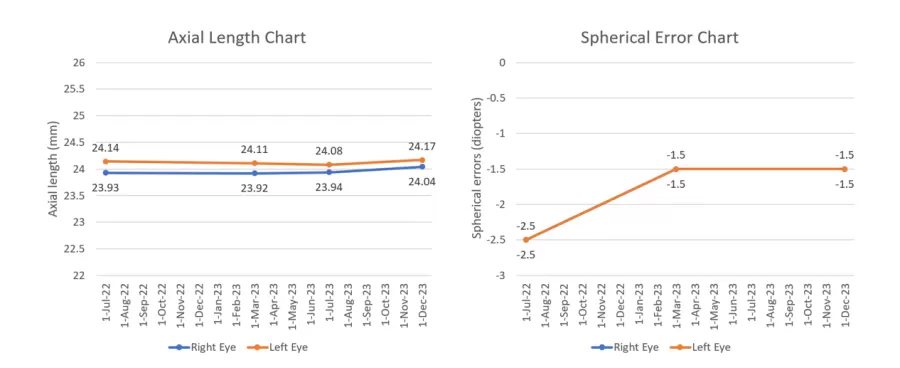
Eighteen months ago, when my son was 9 years old, we initiated his myopia control treatment with spherical errors of -2.5D in both eyes. Initial measurements showed axial lengths of 23.93mm in the right eye and 24.14mm in the left eye. After eight months, a check revealed no myopia progression, with the spherical errors reduced to -1.5D, and the axial lengths remained about the same.
Now, 18 months afterward, our recent follow-up check continued to bring forth encouraging results. My son's myopia continues to be under control without progression. His spherical errors remain at -1.5D in both eyes, and the axial lengths are now at 24.04mm in the right eye and 24.17mm in the left eye. That is a growth of +0.11mm in the right eye and +0.03mm in the left eye over the one and a half years, or 0.07mm/year and 0.02mm/year, respectively.
Results of our myopia control efforts
This year, our journey faced an unexpected twist due to how the U.S. healthcare system works. Our doctor, Dr. B, moved to a clinic outside our insurance coverage, prompting us to switch to Dr. S or pay all expenses out-of-pocket. Recalling our previous experience where we had to temporarily halt Ortho-K for a thorough examination, we paused my son's Ortho-K but continued 0.05% atropine for four weeks before his visit with the new doctor to ensure we could do a full assessment.
Excitingly, the maintenance of his spherical error at -1.5D brought relief, and the growth in axial length was slower than the typical annual increase of 0.3mm for myopic children aged 8-11. Specifically, over the 1.5-year treatment span, there was a growth of +0.11mm in the right eye and +0.03mm in the left eye.
However, after the visit, a closer look uncovered areas for potential improvement. Despite stable spherical errors, his eye axial lengths increased by +0.10mm and +0.09mm compared to our last checkup six months ago.
Slowing or stopping myopia progression means decreasing the rate or stopping spherical error increase while ensuring that axial length growth doesn't outpace that of myopic eyes or is aligned with the typical growth rate for non-myopic children, which is < 0.3mm/year to ≥ 0.09mm/year.1,2
Considering my son started his growth spurt, combined with increased school work and winter, I suspect these factors may contribute to the small growth in his eye axial lengths.3 Furthermore, halting ortho-k treatment for one month may have also contributed to the small increase.
Stopping myopia progression: the proactive approach
As a quick recap, when our son was diagnosed with myopia, my wife and I sought guidance from an optometrist who specializes in myopia control. After careful consideration of my son’s situation, we opted for a proactive approach, combining Ortho-K and a 0.05% low-concentration atropine from the start. This combination targeted two crucial mechanisms—peripheral hyperopic defocus and dopamine release signal pathway—proven to be highly effective in myopia control.
The treatment plan involved nightly Ortho-K use for six nights (9-10 hours) followed by one night of rest, alongside the nightly administration of 0.05% atropine. Despite encountering the blurred near vision side effect initially, leading to adjustments in atropine frequency (initially every other day), the side effect resolved by itself gradually, and we have been using atropine every night since March of this year.
In addition to the medical interventions, we've implemented various lifestyle measures:3,4
- Outdoor Time: After summer but before winter, we achieved more than 4 hours per week or an average of >2 hours daily of outdoor time. However, it reduced to an average of 60-80 minutes per day during shorter daylight hours in December.
- Eye Breaks: Initially, we introduced a 5-minute eye break after every hour of reading or screen time. However, we inadvertently became less vigilant. It's clear that there is room for improvement in adhering to this practice.
- Well-Lit Study Area: Ensuring his study area is well-lit with more than 500 lux brightness using an incandescent light bulb.
- Reading Distance: Maintaining a reading distance of more than an elbow length. That is more than 12 inches or 30 cm.
- Bedtime: Adhering to a bedtime around 9 to 9:30 pm and waking up about 7:00 am. Insufficient sleep duration (< 7 hours), poor sleep quality, and staying up late (after 9:30 pm) are correlated with an increased risk of myopia progression.5
What areas could we improve?
As highlighted earlier, we still have room for improvement. Over the past six months, I have noticed that we were slightly less rigorous when it came to adherence to eye breaks. While my son has taken on more responsibility for managing his own eye breaks, we've noticed lapses in setting timers, resulting in prolonged reading periods. This is especially the case when deeply engaged in schoolwork or personal reading; he often forgets to include essential eye breaks.
Recognizing the potential impact of eye break adherence on stopping myopia progression, my son and I have discussed and devised a PIP – Personal Improvement Plan, which is to enhance adherence to the recommended eye break schedule while shortening the intervals —to 5 minutes for every 30 minutes of close-up work.6 Ultimately, we will do our best to minimize his eye axial elongation, targeting the growth rate to that of non-myopic eyes.
Conclusion
In our 1.5-year myopia journey, stopping myopia progression with a proactive strategy of combination treatment from treatment initiation was effective. This strategy, complemented by lifestyle adjustments, such as increased outdoor time, regular eye breaks, well-lit study environments, and good sleep patterns, has proven effective.
It's important to remember that myopia control is a collaborative effort involving parents, healthcare professionals, and the child. Ongoing communication with the doctor, vigilant monitoring, adjusting the treatment plan as necessary, and fostering healthy eye habits are paramount for success.
By adopting an appropriate myopia treatment with your healthcare professional, you can empower your child to maintain clear vision and succeed in stopping myopia progression.
Want to stay connected on the newest happening? Join me
Facebook group: www.facebook.com/groups/myopia/
Pinterest board: https://www.pinterest.com/clearsightcorner/
Comments