
Some myopia control treatments and circumstances may lead to a temporary reduction in the axial length and/or refractive error, but cannot reverse myopia.
Have you ever wondered if it is possible to reverse myopia? Why do healthcare professionals mainly focus on discussing slowing or halting myopia?
These are questions that may frequently occupy the thoughts of parents who are searching for solutions to manage their children's myopia. This article delves into the concept of reversing myopia, shedding light on what it entails and examining the circumstances that may seem to be the case.
What does it mean to reverse myopia?
Myopia, commonly referred to as nearsightedness, is a refractive error in that distant objects appear blurry while nearby objects are clear. It occurs when the eyeball is excessively long from front to back or when the cornea or lens is overly curved. This leads to light rays entering the eye being focused in front of the retina when ocular accommodation is relaxed.1
Individuals with high myopia often exhibit structural changes in the eye linked to axial elongation, increasing the risk of severe eye complications like myopic macular degeneration, retinal detachment, cataracts, and glaucoma. These complications can be vision-threatening and may require medical intervention.2
So, to reverse myopia would mean an improvement that includes a reduction in axial length, essentially the abnormal structural elongation of the eye, and a reduction in refractive error.
Is it possible for the eye axial length to be shortened?
The anticipated results of myopia control treatments typically involve slowing down or halting the progression of myopia—both in terms of refractive error and axial length. However, the question arises: are there any treatment options demonstrating the potential to shorten the axial length of the eye?
When starting myopia control treatment, it's natural to closely monitor any observed changes. If your child is undergoing one of the following treatments, there may be a chance to notice some axial length reduction, which potentially may also result in a refractive error change. However, it's important to note that, as of now, there is no treatment proven to bring about a permanent change in axial length.
A. Atropine:
In a small-scale, short-term clinical trial published in 2020, the use of topical 0.125% atropine for one week resulted in a positive change in mean refractive error by 1.5 D, accompanied by a mean axial length decrease of 0.016 mm.3 Supported by another study, involving 0.05% atropine, approximately one in six children exhibited initial axial length shortening after treatment. Afterward, their axial length would resume growth but at a slower rate of growth compared to children who did not experience shortening. This suggests that children who have axial length shortening at the start of treatment may respond better and have more favorable outcomes.4
B. Orthokeratology (Ortho-K):
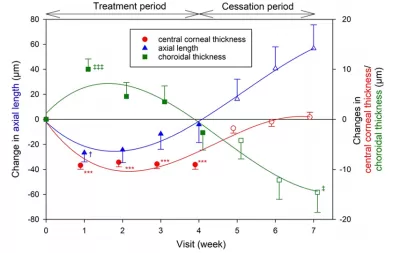
Research suggests when initiating Ortho-K treatment, a reduction in axial length may occur. However, this effect tends to diminish over weeks, possibly attributed to corneal thinning and choroidal thickening.
In a 2019 study, the reduction in axial length was approximately -0.026 mm after one week but returned to baseline after four weeks. Similar to atropine, the reduction could serve as indicators of a child's potential response to Ortho-K treatment -- the more axial shortening at the beginning, the slower the progression of myopia.5
C. Repeated low-level red-light (RLRL) treatment:
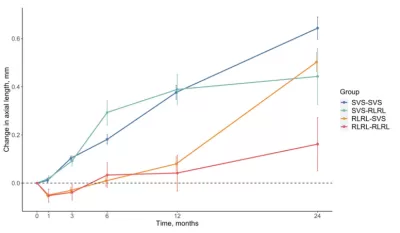
In a 2022 study, which excited the medical community, a new treatment option called the repeated low-level red-light (RLRL) treatment for the first time showed an axial length shortening effect for up to six months. The study encompassing 264 children aged 8 to 13 years and utilizing the new RLRL treatment, results showed that after 6 months of treatment, children experienced a reduction in axial length by 0.08 mm and a decrease in refractive error by 0.2 D.6
In a subsequent two-year follow-up study, an initial improvement in axial length and refractive errors—indicative of the potential for reverse myopia —was observed in the first three months of follow-up. However, despite exhibiting better results than the single-vision control group, these changes returned to baseline level after 6 months.7
Is it possible to reduce refractive error?
It's common and natural to speculate that a reduction in the refractive error implies it is possible to reverse myopia. However, the refractive error, influenced by the optic system, including the cornea, lens, and eye axial length, may exhibit fluctuations or even reductions.8
Further, it is important to note that the structural changes of the eye that are linked to axial elongation are the drivers for the increased likelihood of vision-threatening eye complications.9 Consequently, not requiring glasses or achieving clear vision doesn't necessarily indicate a reduction in the risk of these eye complications.
Let's explore the different scenarios in which one might observe a reduction in the refractive error.
A. Axial length:
A reduction in axial length can lead to improvements in refractive errors, with approximately 0.4 mm of axial length correction corresponding to a one-diopter change. As discussed in the preceding section, several treatment options have shown the potential for temporary—ranging from weeks to months—shortening of the axial length at the initiation of treatment. Consequently, any decrease in refractive error due to axial length reduction is also likely to be of a short-term nature.
B. Accommodative spasms:
The use of cycloplegic refraction to alleviate accommodative spasm is crucial for accurately measuring refractive errors, as a difference of 0.3 to 0.8 diopters may be observed.10 Accommodative spasms may contribute to the fluctuations seen in refractive error measurements between clinic visits. Considering that the majority of eye clinics in the US do not employ cycloplegic refraction, providing sufficient eye breaks, practicing eye exercises, or even not being in a state of anxiety during eye examination may contribute to a reduction in the refractive error.8
C. Emmetropization:
Emmetropization is the natural process during postnatal development in which the refractive components and axial length of the eye find a harmonious balance. Most infants typically begin with hyperopia (farsightedness) and gradually progress towards emmetropia—a state without any refractive error.11
In children without myopia, their eyes are anticipated to undergo normal growth from birth until around the age of 12. During the school-aged years, the eye grows at a rate of about 0.1 to 0.2 mm per year. As children enter their teenage years, this growth decelerates to around 0.1 mm per year and eventually ceases in the early teens.11
This suggests that if the growth of eye axial length is either halted or slower than emmetropization, it may lead to a reduction in refractive errors.
Conclusion
In exploring the possibility of reversing myopia, it's crucial to recognize that myopia may exhibit temporary and apparent reversals. Atropine, Ortho-K, and RLRL treatment might provide transient reductions in axial length, lasting from weeks to months, resulting in fluctuations and occasional improvements in refractive error. Nevertheless, the fundamental message remains clear—myopia cannot be reversed.
Want to stay connected on the newest happening? Join me @
Facebook group: www.facebook.com/groups/myopia/
Pinterest board: https://www.pinterest.com/clearsightcorner/
Comments