
An overview of different treatments available to help my kid prevent his myopia from progressing - a parent’s perspective (US).
How are the lifestyle changes working?
In my prior post on June 10th, I discussed why I thought it’s important to keep my son’s myopia in check and how I plan to help keep his condition under control.
Since then my son and I have started some lifestyle changes that my son can keep to – with empathetic, caring, motherly, and constant reminders from me and his mom of course. The outdoor activity tracker was a great supportive tool for my son. And he started having omega-3 supplements since he really doesn’t like having fish.
His smart device use was kept under 30 min per day. He used voice assistants around the house to remind himself to relax his eye. (20 mins was hard for him to keep track so we adjusted it to every 30min for 30 seconds, even though it is not evidence-based.)
In general, I am pretty happy that it seems he could maintain the lifestyle change with some reminders and encouragement.
How did I evaluate myopia control options?
On the non-lifestyle part, there were some hiccups. We still don’t have an eye doctor focused on pediatric myopia control to work with.
To better prepare for the upcoming discussions, I spent some time understanding the treatment options and thought some of you may find it useful.
I took note and summarized the effectiveness of myopia progression based on a meta-analysis of 16 interventions (Huang 2016), then adapted a 2020 Cochrane database review plus a couple of individual research publications for newer treatment options that were not included originally.
How to evaluate myopia progression?
Reading through the literature, I found it confusing trying to figure out how the risk of myopia progression reduction was calculated or how that translates to what I may see from my son’s eye examination results. Further, I found it easier to have a holistic view of the treatment effects through an understanding of the natural history of myopia progression.
Here is a summary of my learning.
A human eye grows extensively after birth. A newborn baby's eye has an axial length of 16-18 mm. It will grow to 22-25 mm in adulthood. And the axial length grows on an average of 0.1 to 0.2 mm/yr between the age of 6 to 14 years old.
The average natural progression rate of myopia in children of the European population was estimated to be -0.55 D/yr and -0.82D/yr in Asians. From a different study, the average axial length growth was 0.25 mm/yr for children of white ethnicity and 0.30 mm/yr for Asian children. Myopic eyes grew faster and for a longer duration. The estimated progression rate in all studies was dependent on the age with decreasing progression as age increased.
There were two common measures of reporting myopia progression - change in refractive error and axial length.
The refractive error is reported in a negative value and in diopter (D). A positive value of change in the refractive error means that it is progressing slower than the comparator. (The relative effect in the overview was defined using the same approach and cut-offs as the Huang 2016 paper).
- Strong effect: ≥0.50 D/yr
- Moderator effect: 0.25 to 0.50 D/yr
- Weak effect: 0 to 0.25 D/yr
- Ineffective: ≤0 D/yr
Since myopia progression is accompanied by axial length increases – a plus in value, a negative change in axial length means that it is increasing slower than the comparator. And, the relative effect on the change in axial length was defined below.
- Strong effect: ≤-0.18 mm/yr
- Moderator effect: -0.09 to -0.18 mm/yr
- Weak effect: 0 to -0.09 mm/yr
- Ineffective: ≥0 mm/yr
Treatment options to prevent myopia from progressing
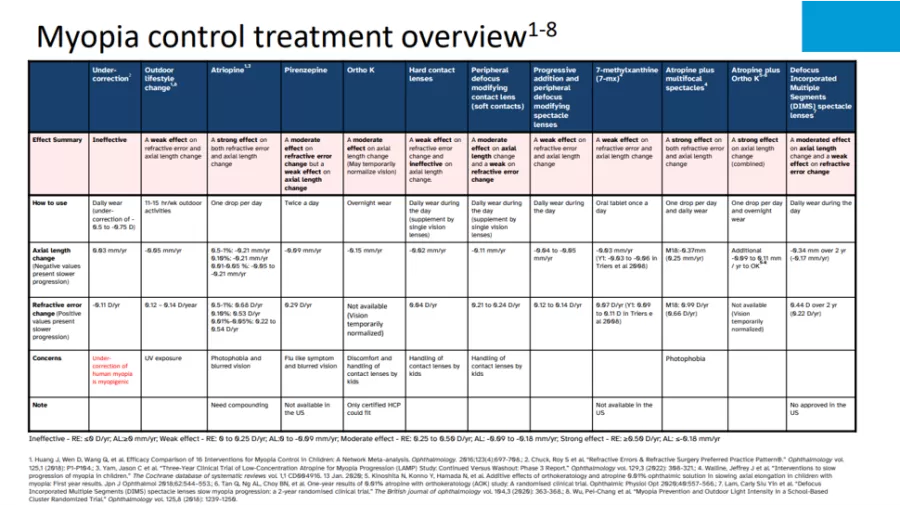
(This table is available for download )
1. Outdoor time
- Outdoor time has a weak effect on both refractive error and axial length change. But the cost is minimal to none.
Daylight, which may lead to hormone release and impacts the growth of the eyes, seems to be how more outdoor activities help slow down the progression of myopia. This means not only activities under the sun but also in the shed with sufficient brightness.
Many studies indicated outdoor time reduces the likelihood of myopia onset. However, whether outdoor time could prevent myopia progression is still a topic of discussion. Some studies show positive results, but others are inconclusive.
Considering that outdoor activities (11-15 hrs/week) only had a weak effect on refraction and axial length change. I think it might contribute to why some studies were inconclusive.
In light of this learning, I still believe that outdoor activities may continue to be an important part of myopia control for my son – as the assist leader.
2. Atropine and other pharmaceutical agents
Atropine eye drop
- Atropine has a strong effect on both refractive error and axial length change. This is the most effective treatment with a relatively medium cost-to-effect ratio.
Atropine is an antimuscarinic, a subtype of an anticholinergic agent, which induces dilation of the pupil. However, the exact mechanism of action for slowing the progression of myopia is not well understood.
Several reports indicated that low-dose atropine (0.01% to 0.05%) can effectively help slow myopia progression while minimizing the rebound effect and some of the side effects, including light sensitivity, blurry vision, and increase pupil size.
Here in the US, there is no commercially available low-dose atropine for myopia control. But, they can be ordered from a compounding pharmacy - not as straightforward. The cost seems to be about US$60-100 for each month of supply.
“Did you know that Women used to use juice of the berries of the nightshade containing atropine to enlarge their pupil for cosmetic reasons?
Other pharmaceutical agents
Even though pirenzepine and 7- methylxanthine(7-mx) are two interesting alternatives to atropine due to pirenzepine’s reduced light sensitivity risk and the oral dosage form of 7-mx, they are not available in the US.
3. Orthokeratology and hard contact lenses
Orthokeratology (Ortho-K)
- Ortho-K has a moderate effect on axial length change. It corrects myopia temporarily. It also comes with a relatively higher cost and may be more suitable for slightly older kids.
Orthokeratology, also known as Ortho-K, uses custom-designed gas permeable contact lenses to reshape the cornea. By wearing the contact lenses each night (or several hours a day), your kid may not need vision correction during the day. However, some children with high myopia may still need glasses to correct for residual refractive error.
Studies indicated that Ortho-K lenses could be combined with atropine treatment and had a strong effect on axial length and refraction change, and provided additional efficacy when compared to Ortho-K monotherapy.
Overall, Ortho-K is a safe and effective method of slowing the progression of myopia in children. Ortho-K lenses, like any contact lenses, may lead to an increased risk of eye infection. An important consideration when evaluating if Ortho-K is appropriate is if your kid is mature enough to follow instructions on ensuring hygiene and proper handling of the lenses.
The fitting process for Ortho-K is more exact than for soft contact lenses. It may take a few clinic visits to ensure proper fitting.
The typical first-time cost of Ortho-K treatment usually runs around US$1,200 to US$2,000, depending on the refractive error. Complex cases may cost up to US$5,000. This includes an eye exam, the fitted lenses, and a few follow-ups. Then, the costs for the second and following years may come to around US$650 per year. An additional cost to include is the cleaning and disinfecting solutions, which will be about US$150 to 200 per year. (This is the cost in the US and around my area. Different countries and regions may be substantially different.)
Hard contact lenses (Rigid gas permeable contact lenses)
- Hard contact lenses have a weak effect on refractive error change and are ineffective on axial length change. I am considering other options first.
Even though Ortho-K lenses use the same rigid gas permeable materials, hard contact lenses are intended to correct the refractive errors and are worn during the day. Due to they are ineffective in slowing axial length, I would consider other options first.
4. Soft contact lenses
Peripheral defocus modifying contact lenses
- Peripheral defocus modifying (PDM) contact lenses have a moderate effect on axial length and refractive error change. The cost is less expensive than Ortho-K and they are more widely available.
There are several types of design including dual focus, bifocal, and defocus incorporated. Soft contact lenses help correct refractive error when wearing and simultaneously slow down myopia progression.
Similar to Ortho-K, an important consideration when evaluating if soft contact lenses are appropriate is if your kid is mature enough to follow instructions on ensuring hygiene and proper handling of the lenses, i.e., how to put it in or what to do if it falls out.
The price is around $1,000 to 1,500 per year (dual focus type). The cost of backup glasses should be added.
5. Spectacle lenses
Defocus Incorporated Multiple Segments (DIMS) spectacle lenses
- DIMS spectacle lenses have a moderated effect on axial length change and a weak effect on refraction change. Unfortunately, it is not available in the US.
DIMS seems to be an option with a similar or slightly better effect vs peripheral defocus modifying contact lens on the axial length change. However, they are not available in the US.
Progressive addition (PA) and peripheral defocus modifying (PDM) spectacle lenses
- These spectacle lenses have a weak effect on axial length and refraction change. I am considering other options first.
These spectacles may be used as an adjunct to other therapy or combination therapy.
If your kid wears contact lenses, these spectacles could be the backups or for residual correction of Ortho-K treatment.
Studies indicated that PDM spectacle lenses could be combined with atropine treatment and had a strong effect on axial length and refraction change, and they provide additional efficacy when compared to spectacle monotherapy.
Final thoughts
This overview is based on treatment options evaluated through clinical trials, and that are or may become available in the US. Further, due to a lack of valid studies, I didn’t include a few other alternative treatments that I came across, such as visual training or acupressure.
I can’t emphasize more that it is important to work with your eye doctor to determine the most appropriate treatment for your kid. At the end of the day, each kid’s situation is different. What may work for one may not work for another.
Until then, off to the swimming pool to support my son banking some daylight time.
Want to stay connected on the newest happening? Join me @
Facebook group: www.facebook.com/groups/myopia/
Pinterest board: https://www.pinterest.com/clearsightcorner/
Comments